

Insulin Clearance in Obesity and Type 2 Diabetes
- PMID: 35054781
- PMCID: PMC8776220
- DOI: 10.3390/ijms23020596
Insulin Clearance in Obesity and Type 2 Diabetes
Abstract
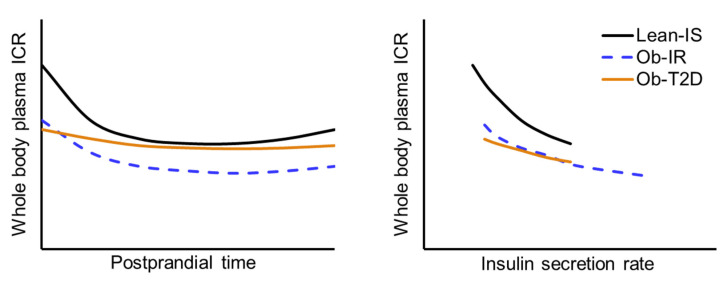
Plasma insulin clearance is an important determinant of plasma insulin concentration. In this review, we provide an overview of the factors that regulate insulin removal from plasma and discuss the interrelationships among plasma insulin clearance, excess adiposity, insulin sensitivity, and type 2 diabetes (T2D). We conclude with the perspective that the commonly observed lower insulin clearance rate in people with obesity, compared with lean people, is not a compensatory response to insulin resistance but occurs because insulin sensitivity and insulin clearance are mechanistically, directly linked. Furthermore, insulin clearance decreases postprandially because of the marked increase in insulin delivery to tissues that clear insulin. The commonly observed high postprandial insulin clearance in people with obesity and T2D likely results from the relatively low insulin secretion rate, not an impaired adaptation of tissues that clear insulin.
Keywords: insulin clearance; insulin extraction; insulin secretion.
Conflict of interest statement
The authors report no conflict of interest relevant to this article.
Figures
Similar articles
-
β Cell function and plasma insulin clearance in people with obesity and different glycemic status.J Clin Invest. 2022 Feb 1;132(3):e154068. doi: 10.1172/JCI154068. J Clin Invest. 2022. PMID: 34905513 Free PMC article. Clinical Trial.
-
Disturbances of basal and postprandial insulin secretion and clearance in obese patients with type 2 diabetes mellitus.Horm Metab Res. 2012 Jan;44(1):60-9. doi: 10.1055/s-0031-1295414. Epub 2011 Dec 28. Horm Metab Res. 2012. PMID: 22205571
-
Beta-cell function and mass in type 2 diabetes.Dan Med Bull. 2009 Aug;56(3):153-64. Dan Med Bull. 2009. PMID: 19728971
-
Metabolism and insulin signaling in common metabolic disorders and inherited insulin resistance.Dan Med J. 2014 Jul;61(7):B4890. Dan Med J. 2014. PMID: 25123125 Review.
-
Obesity, insulin resistance, and its link to non-insulin-dependent diabetes mellitus.Metabolism. 1995 Sep;44(9 Suppl 3):18-20. doi: 10.1016/0026-0495(95)90314-3. Metabolism. 1995. PMID: 7674911 Review.
Cited by
-
Effect of dietary approaches to stop hypertension and curcumin co-administration on glycemic parameters in polycystic ovary syndrome: An RCT.Int J Reprod Biomed. 2024 Nov 14;22(9):689-700. doi: 10.18502/ijrm.v22i9.17473. eCollection 2024 Sep. Int J Reprod Biomed. 2024. PMID: 39618714 Free PMC article.
-
Polycystic Ovary Syndrome as Metabolic Disease: New Insights on Insulin Resistance.touchREV Endocrinol. 2023 May;19(1):71-77. doi: 10.17925/EE.2023.19.1.71. Epub 2023 May 17. touchREV Endocrinol. 2023. PMID: 37313240 Free PMC article. Review.
-
Critical Evaluation of Indices Used to Assess β-Cell Function.Diabetes. 2024 Mar 1;73(3):391-400. doi: 10.2337/db23-0613. Diabetes. 2024. PMID: 38015795 Free PMC article.
-
Standardized Ethanol Extract of Cassia mimosoides var. nomame Makino Ameliorates Obesity via Regulation of Adipogenesis and Lipogenesis in 3T3-L1 Cells and High-Fat Diet-Induced Obese Mice.Nutrients. 2023 Jan 25;15(3):613. doi: 10.3390/nu15030613. Nutrients. 2023. PMID: 36771320 Free PMC article.
-
Succinylation enables IDE to act as a hub of larval tissue destruction and adult tissue reconstruction during insect metamorphosis.Sci Adv. 2025 Feb 7;11(6):eads0643. doi: 10.1126/sciadv.ads0643. Epub 2025 Feb 5. Sci Adv. 2025. PMID: 39908369 Free PMC article.
References
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
