

Abstract
Antibody-mediated rejection has become critical clinically because this form of rejection is usually unresponsive to conventional anti-rejection therapy, and therefore, it has been recognized as a major cause of allograft loss. Our group developed experimental animal models of vascularized organ transplantation to study pathogenesis of antibody- and complement-mediated endothelial cell injury leading to graft rejection. In this review, we discuss mechanisms of antibody-mediated graft rejection resulting from activation of complement by C1q- and MBL (mannose-binding lectin)-dependent pathways and interactions with a variety of effector cells, including macrophages and monocytes through Fcγ receptors and complement receptors.
Keywords: Alloantibody, Complement, Ig knockout mice, Cardiac rejection, vWf, C4d, MBL, Fcγ and complement receptors, Endothelial cells, Macrophages
Significance of antibody and complement in allotransplantation
Alloantibody contributes significantly to rejection of heart transplants by activation of complement and interactions with a variety of effector cells, including macrophages and monocytes through Fcγ receptors (FcγRs) and complement receptors (CRs). Alloantibody-mediated organ rejection (AMR) has become clinically critical because this form of rejection is usually unresponsive to conventional anti-rejection therapy. Therefore, AMR is one of the greatest therapeutic challenges in transplantation. It has recently been recognized as a major cause of allograft loss in populations such as patients with previous open-heart surgery, multiple transfusions and multiparous females.
The potential for complement to function as an effector in graft rejection has been recognized since early experiences with clinical xenografts and allografts. Hyperacute rejection was a frequent occurrence in allografts before tests were devised to screen potential recipients for circulating antibodies to the prospective donor [1]. This type of rejection occurs immediately upon perfusion of the transplants with the blood of the recipient. Antibodies in the blood of the recipient bind to the vascular endothelium of the transplant and activate complement, which results in neutrophil infiltration, vascular disruption, hemorrhage, fibrin deposition and platelet aggregation. Tests for donor-specific antibodies have almost eliminated hyperacute rejection. The possibility that antibodies and complement contributed to acute or chronic forms of rejection was not widely appreciated until more sophisticated reagents were developed to demonstrate complement deposition in diagnostic biopsies from organ transplants [2-4].
Clinically recognized antibody-mediated rejection
The contribution of antibody and complement to acute and chronic forms of graft failure is an area of active investigation [5-8]. As of 2009, more than 30% of patients on the transplant waiting list were considered sensitized to HLA antigens. The number of sensitized patients with anti-HLA antibodies has continued to increase since 1994 (12,808 in 1994 vs. ~25,000 in 2009, the organ procurement and transplantation network (OPTN) data [http://optn.transplant.hrsa.gov/]). These patients may remain on waiting lists and require dialysis for prolonged periods of time. Such patients experience an enormous financial and emotional burden while maintained on dialysis. With this ever growing number of sensitized patients waiting for transplants, there is an immediate need to use organs from ABO- and HLA-incompatible living donors and expanded paired-kidney exchange programs. Therefore, it is essential to design successful strategies that inhibit the injurious effects of antibodies.
In the light of growing numbers of patients on waiting lists and a shortage of organs, high levels of circulating antibodies to HLA and ABO incompatibility remain the two major obstacles for optimal use of organs for successful transplantation, especially kidneys from living donors. Therefore, AMR and its treatment is one of the greatest therapeutic challenges in transplantation. It is critical to understand the mechanisms by which antibodies and complement modify cellular responses, because vital clinical decisions are based on the findings of complement activation products in diagnostic biopsies.
Although current desensitization protocols have enabled transplantation across donor-specific antibody barriers in a growing number of cases [9-14], these protocols are neither consistently efficacious nor standardized. It reflects an incomplete understanding of the pathogenesis of alloantibody-induced injury as a major cause of allograft loss. Furthermore, patients treated with these modalities persist in having a high risk of multiple AMR episodes.
The Johns Hopkins Comprehensive Transplant Center directed by Dr. R. Montgomery has pioneered a clinical protocol that removes both donor-specific antibodies to HLA and A or B blood group antigens permitting the successful renal transplantation in highly sensitized and ABO incompatible patients [13, 15, 16].
In 2004, Montgomery’s group reported the first three successful renal transplantations across a positive cross-match and ABO incompatibility [13, 15]. Almost a year after transplantation, all these patients enjoyed well-functioning kidneys, maintained negative cross-match, but stable low titer of isoagglutinin and continuous positive staining for C4d, without histological evidence of acute antibody-mediated or chronic injury. This phenomenon, when transplants function very well despite reemergence of ABO antibodies, is defined as tissue accommodation, an acquired resistance to immune-mediated injury [17-19]. The possible mechanisms involved in accommodation will be discussed later in this review in the context of data from in vitro experiments.
The rationale for the use of C4d as a marker for AMR
Data from several transplantation centers [2, 20-23] indicate that complement split products such as C4d and C3d are deposited on the vascular endothelium in a significant number of acute antibody-mediated rejections of renal and cardiac transplants [24-26].
These rejections are categorized as antibody-mediated rejection when the biopsies contain marginated neutrophils or monocytes and donor-specific antibodies are detected in the circulation. The incidence of AMR associated with the presence of C4d in biopsies varies from about 1% to more than 50% depending on the proportion of sensitized patients in the study [24, 27-29].
Currently, C4d has been adopted as a marker of antibody-mediated rejection [22]. The justification for the selection of C4d, a split product of C4, as a marker for AMR comes from its position in the cascade of complement activation. There are three main pathways of complement activation, the classical, mannose-binding lectin (MBL) and alternative. Each pathway produces C3 convertase, which enzymatically cleaves the central C3 component of the complement system allowing to continue complement cascade as antibody disengages from the surface of the cell through generation of C5 convertase and C5 split products followed by the membrane attack complex (MAC) formation (Fig. 1). However, only the classical and MBL pathways are known to involve the C4 component of complement positioned before C3 in cascade of complement activation.
Fig. 1. C4 as a merge point of classical and MBL pathways of complement activation by antibodies.
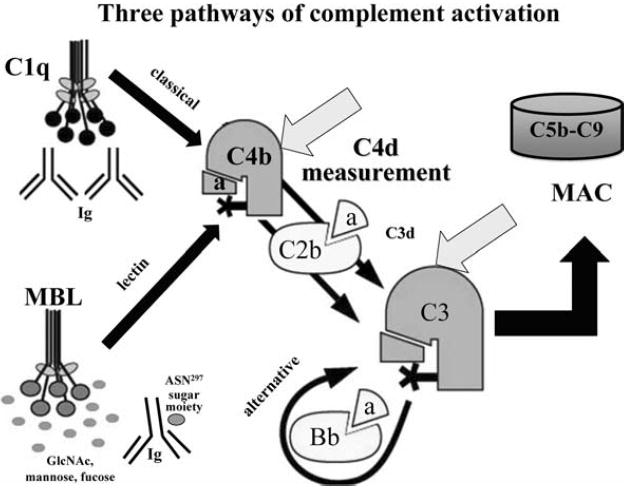
The complement cascade can be activated through three different pathways: the classical (involving C1, C4 and C2) leading to formation of enzymatic molecule C4b2a, the C3 convertase, MBL lectin-dependent pathway and alternative, which is initiated by hydrolyzed C3 and factor B producing alternative pathway C3 convertase, C3bBb. Generation of C3 convertase allows the formation of C5 convertase which is followed by formation a tubular structure of the C5b-9 terminal complement complex, membrane attack complex (MAC). Antibodies activate the complement system primarily through the classical pathway involving C1, which is composed of C1q that binds to antibody, and two C1r and C1s proteases. MBL is associated with MASP-1, 2, 3 serine proteases and initiates the lectin pathway of complement activation through binding to carbohydrates on microorganisms, IgM and some classes of IgG. Both, C1r2s2 and MASP proteases enzymatically cleave C4 into two fragments—C4a and C4b. The larger C4b generates C4d fragment, which is the end product of C4 activation. Both, C4b and C4d have the unusual capacity to form a covalent bond with a hydroxyl or amino group on the closest protein or carbohydrate, e.g., endothelial cell membrane or antibody
Antibodies activate the complement system primarily through the classical pathway involving C1, which is composed of C1q that binds to antibody, and two C1r and C1s proteases. MBL is associated with MASP-1, 2, 3 serine proteases and initiates the lectin pathway of complement activation through binding to carbohydrates on microorganisms, IgM and some classes of IgG. Both, C1r2s2 and MASP proteases enzymatically cleave C4 into two fragments—C4a and C4b. The larger C4b generates C4d fragment, which is the end product of C4 activation. Both, C4b and C4d have the unusual capacity to form a covalent bond with a hydroxyl or amino group on the closest protein or carbohydrate, e.g., vascular endothelial cell membrane or antibody (Fig. 1).
Experimental models of antibody-mediated rejection
The recent growing interest in antibody-mediated rejection has stimulated the development of in vivo and in vitro experimental models to study antibody and complement in acute and chronic rejection. At an NIH-sponsored conference in April 2003, transplantation experts continued to acknowledge the necessity to assess innovative treatment protocols and to develop research tools for studying antibody-mediated rejection.
The major interest of our laboratory is development of experimental models of vascularized organ transplantation to study pathogenesis of antibody- and complement-mediated graft injury and rejection. Our studies promote organ transplantation by contributing to understanding of antibody- and complement-induced mechanisms of graft injury. The ultimate goal of our studies is to translate findings from experimental models to studies using clinical samples from patients undergoing antibody-mediated rejection with a long-term goal of designing novel treatment protocols.
In vitro and in vivo experiments have demonstrated multiple mechanisms by which antibodies and complement can intensify macrophage, B-cell and T-cell responses [30-33]. A limited number of experiments in animals genetically deficient for immunoglobulins or complement components have revealed that some of these mechanisms may have significant effects on the survival of hearts [34] and lungs [35, 36] in C6-deficient rats, skin in C3-, C4- and C5-deficient mice [37], kidneys in C3- and C4-deficient mice [32, 38, 39], and hearts in immunoglobulin knockout (Ig-KO) mice [40-43] or in RAG1 mice [44].
Cardiac allotransplantation in mice as a model of antibody-mediated rejection
In our laboratory [40-42], we have established a reliable model of cardiac transplantation in Ig-KO mice to demonstrate a causative role of antibody in acute allograft rejection.
Cardiac allografts from B10.A (H-2KkDd) donors survive longer in C57BL/6 Ig-KO (H-2b) recipients, which do not produce antibodies on their own, than in their WT counterparts [40, 45]. B10.A cardiac allografts were rejected within 7–14 days in WT C57BL/6 recipients. In contrast, 85% of the cardiac allografts from B10.A donors survived more than 14 days in C57BL/6 Ig-KO recipients, with over half surviving more than 50 days after transplantation (P < 0.0001) by log-rank test in Kaplan–Meier plot analysis.
We used this model to perform passive transfer experiments to Ig-KO recipients of cardiac allografts to probe the effect of low and high doses of specific to MHC class I (H-2Kk present on B10.A cells) monoclonal antibodies representing different mouse IgG subclasses on graft survival. We used a panel of mAbs: IgG2a (16-3-1N) anti-H-2Kk, IgG2a (16-1-2N) anti-H-2KkDk, IgG2b (15-1-5P) anti-H-2KkDk and IgG1 (AF3-12.1.3) anti-H-2Kk. In a mouse model of heart transplantation, we have shown that passive transfer of high doses of IgG2b complement-activating antibodies to C57BL/6 Ig-KO recipients significantly shortened the survival time of the allografts, which were rejected within 48 h after injection of alloantibodies [40, 41]. This effect was dose dependent, and low doses of complement-activating alloantibodies did not accelerate graft rejection. In contrast, non-complement-activating IgG1 alloantibodies administered over a wide range of doses did not accelerate graft rejection. Unexpectedly, cardiac allografts were vigorously rejected within 48 h in mice that had been given low doses of complement-activating alloantibody in combination with a high dose of non-complement-activating alloantibody. This novel finding brought us to conclusion that complement-activating and non-activating alloantibodies can synergize to accelerate graft rejection.
von Willebrand factor (vWf) and P-selectin mediate endothelial cell injury in vivo
Clinically, rejection of human cardiac transplants is associated with an increased expression of P-selectin and vWf on the vascular endothelium [46], capillary Ig and complement deposition, the presence of intravascular CD68 positive macrophages and fibrin staining in vessels of grafts with AMR [27, 47].
In physiological conditions, endothelial cells constitute an anti-inflammatory barrier between the circulation and the extravascular tissues, but activated endothelial cells are transformed into a procoagulant, chemoattractive and adhesive interface that promotes inflammation. Many recent studies have described the crucial role of intravascular platelet aggregates in clinical and experimental models of antibody-mediated rejection [35, 40, 48-50]. Recently, Morrell et al. and Kirk et al. [51, 52] extensively reviewed the role of platelets and the mechanisms promoting interactions between platelets, endothelial cells, macrophages and lymphocytes in the context of organ antibody-mediated rejection.
vWf is an important link between endothelial cell activation and platelet aggregation. Endothelial cells synthesize vWf as 250 kDa subunits that are stored as multimers ranging up to 10,000 kDa in Weibel-Palade bodies. The immediate effect of endothelial cell activation is the retraction of the plasma membrane from the underlying substrate [53, 54] and the release of preformed vWf and P-selectin from cytoplasmic Weibel-Palade bodies to the cell surface [55]. The multivalency of the large multimers released from the Weibel-Palade bodies leads to extremely effective activation and aggregation of platelets [56]. Secreted vWf interacts specifically with two types of transmembrane receptors: (1) the GPIb (CD42b) receptor on platelets and (2) the integrin-type receptors, including the GPIIb/IIIa (CD41/CD61) complex on platelets and the vitronectin receptor on endothelial cells [57].
Our extensive studies performed in collaboration with groups led by Craig Morrell and Charles Lowenstein [49, 52, 58, 59] provided insights into the role of antibody- and complement-mediated endothelial cell injury leading to vascular inflammation and graft rejection. Morrell et al. [49] have shown in the model of skin transplantation in mice that MHC-specific antibodies induce platelet activation and rolling in vivo. Repeated injections of antibodies result in sustained platelet–endothelial interactions and vascular pathology, including vWf release, formation of thrombi and complement deposition. Increased interaction of platelets and leukocytes with endothelium was visualized by the presence of fluorescent-labeled platelets in real time and decreased cell velocity [49]. Lowenstein’s group documented that antibodies to human HLA induce skin graft rejection by triggering endothelial exocytosis, release of vWf and externalizing P-selectin, which in turn induce platelet aggregation and leukocyte trafficking [58, 59].
In our model of cardiac allografts in Ig-KO mice passively transferred with high doses of complement-activating antibodies acute antibody-mediated rejection was also accompanied by extensive aggregates of platelets that stained intensively for vWf and P-selectin [40]. These platelet aggregates occluded the arteries, capillaries and veins of rejected allografts. In contrast to the effect of complement-activating alloantibodies, vWf remained confined to the storage granules of the endothelial cells in non-rejected cardiac allografts treated with even high doses of IgG1 [40].
P-selectin that is released from endothelial cell α-granules not only initiates the adhesion of monocytes and platelets to the endothelium, but also costimulates the production of inflammatory mediators by endothelial cells [60-62]. Engagement of P-selectin on endothelial cells or platelets with the PSGL-1 ligand expressed by leukocytes results in the activation of endothelial cells. Subsequently, activated endothelial cells produce IL-1-α, IL-8, RANTES and monocyte chemotactic protein 1 (MCP-1) to recruit neutrophils and monocytes to the site of injury [63, 64]. We have shown that all these cytokines/chemokines were upregulated in rejected hearts in Ig-KO mice passively transferred with rejecting doses of antibodies [65].
Our experiments in C6-deficient rats also indicate that the MAC is critical for this type of endothelial response in allografted hearts or lungs [35, 50, 66]. Only moderate expression of P-selectin and minimal platelet aggregation was found in C6-deficient hearts transplanted into C6-deficient recipients [50, 66]. Likewise, C6-deficient lungs were characterized by quiescent vascular endothelial cells, with minimal vWf release and no evidence of alveolar hemorrhage or edema [35]. Numerous in vitro experiments confirmed a critical role of MAC formation in endothelial cell activation. Specifically, purified components of MAC have been shown to cause endothelial cells to release vWf as well as to synthesize IL-8, MCP-1, P-selectin, E-selectin and ICAM-1 [53, 63, 64, 67-69]. α-Granules of activated platelets contain many chemokines, such as MIP-1-α, RANTES, MCP-3 and PF4 (CXCL4) [70, 71]. These chemokines attract and activate macrophages and lymphocytes to the site of injury. Migration and maturation of antigen-presenting cells is promoted by platelet-derived ICAM-1, P-selectin, IL-1, IL-6 and GM-CSF [70, 71].
Intragraft deposition of C4d in cardiac transplants in Ig-KO mice
Immunohistochemical stains for C4d on cardiac allograft tissues using our newly developed polyclonal antibody specific to mouse C4d confirmed that antibody-mediated cardiac allograft rejection in vivo correlates with the extent of C4d deposition in grafts [42]. Ig-KO mice injected with high doses of non-complement-activating IgG1 antibody to MHC class I alone showed no staining for C4d. Similarly, cardiac allografts from Ig-KO mice given a low dose of complement-activating IgG2b antibody alone were also negative for C4d. In contrast, cardiac allografts from Ig-KO mice treated with a high dose of IgG2b showed significant deposition of C4d on the vascular endothelium in arteries and capillaries. Likewise, mice injected with a low dose of IgG2b combined with a high dose of IgG1 had significant deposition of C4d on the vascular endothelium of the graft. The pattern and extent of C4d staining in both rejecting groups were similar to the staining in WT allograft recipients (Fig. 2 in [42]). Furthermore, our model of antibody-dependent cardiac allograft rejection in Ig-KO mice demonstrated clearly that IgG1 can augment the pathogenic effects of a subthreshold dose of IgG2b and produce pathology comparable to that one seen in WT recipients [41, 42].
C4d deposition in rejected hearts was correlated with high levels of MCP-1 as well as IL-6 and IL-1-α mRNA transcripts measured by real-time PCR [65]. In contrast, the levels of these cytokines were remarkably lower in the graft recipients treated with low doses of complement-activating or high doses of non-complement-activating alloantibodies, which did not cause acute antibody-mediated rejection. These findings led us to conclude that upregulation of C4d along with pro-inflammatory MCP-1, IL-6, IL-1-α within the grafts is relevant to antibody-mediated rejection and may be caused by complement-activating as well as non-activating antibodies.
The unique ability of IgG1 to enhance complement activation in cardiac transplants in Ig-KO mice
In an attempt to investigate the mechanism of IgG1-mediated enhancement of complement activation, we tested in vitro IgG1 mAb AF3-12.1.3, which has been used in our in vivo studies. This particular IgG1 AF3-12.1.3 mAb did not cause any measurable C3d or C4d deposition on endothelial or lymph node cells over a wide range of doses. This is important because both complement-activating and non-complement-activating mouse IgG1 antibodies have been reported [72-74]. These differences have been attributed to the structure of the variable regions of IgG1 [75, 76]. Moreover, IgG1 has been reported to augment IgG2b- and IgG2a-induced complement-mediated lysis of erythrocytes [77]. The mechanism of this synergy is incompletely understood, but it may involve steric interference of C1 inhibitor or the ability to provide more cellular membrane binding sites for C4b and C3b.
The involvement of MBL in antibody-mediated tissue injury and graft rejection
MBL is an important protein of the innate immune system [78] and is known to bind to carbohydrates on microorganisms. Also, some classes of Ig, namely, IgM [79, 80] and IgG [81] have been reported to bind MBL.
The exact mechanism by which MBL binds to glycoforms of IgG subclasses is not known. IgM and IgG antibodies are glycoproteins that contain a branched sugar structure (N-linked glycan) attached to the asparagine 297 residue within the Fc fragment of the antibody. The level of glycosylation of this glycan is crucial for the pro- or anti-inflammatory effector functions of antibody resulting in complement activation and interaction with Fc and complement receptors (will be further discussed in the next section).
In the model studied in our laboratory (Fig. 2), we hypothesized that alloantibodies bound to endothelial cells initiate complement activation through the C1q- and MBL-dependent pathways. MBL binds to carbohydrates on the Fc fragment of antibodies. Since both C1q and MBL cleave C4 producing enzymatically active C4b product deposited on endothelial cells (Fig. 1), antibody-mediated complement activation leads to endothelial cell injury and ultimately graft rejection.
Fig. 2. A model linking antibody and complement to endothelial cells, macrophages, T and B cells.
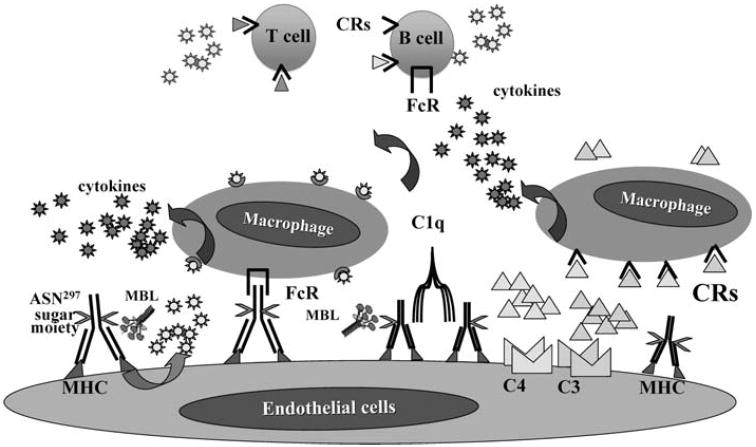
In this model, alloantibody bound to endothelial cells initiates complement activation through classical- and MBL-dependent pathways and activates macrophages via complement, CRs and FcγRs to produce IL-1-α, IL-1-β, IL-6 and TNF-α. Oligosaccharides attached to the asparagine 297 residue on the Fc fragment of antibody modulate the function of IgG subclasses, especially activation of complement and interaction with FcγRs expressed on mononuclear cells
In our mouse model of antibody-mediated cardiac allograft rejection, we demonstrated that complement activation and deposition of C4d results from the synergistic effect of complement-activating IgG2a or IgG2b with non-complement-activating IgG1 alloantibodies. In vitro experiments confirmed the potential for IgG1 to modify complement activation by IgG2a or IgG2b. In these experiments, we found that IgG1 synergized with complement-activating alloantibodies because the addition of increasing doses of IgG1 to lymph node cells sensitized by low doses of complement-activating antibodies augmented deposition of C4d on target cells [42].
Furthermore, we have proven that MBL plays a role in the synergistic activation of complement by the combination of complement-activating and non-activating alloantibodies using sera from C1q-KO, MBL-A/C-KO or mixed 1:1 C1q-KO + MBL-A/C-KO mice [42]. The absence of C1q in serum completely eliminated the ability of high doses of both IgG2a or IgG2b alone to deposit C4d on the cell surface, as well as the ability of IgG1 to synergize with low doses of IgG2a or IgG2b to deposit C4d [42]. Similarly, the absence of MBL significantly decreased C4d deposition by high doses of IgG2a or IgG2b and also by combinations of IgG1 with low doses of IgG2a or IgG2b. Reconstitution of the MBL and C1q deficiency by combining MBL-deficient serum with C1q-deficient serum restored the ability of a high doses of IgG2a or IgG2b alone, as well as both IgG1 + IgG2a and IgG1 + IgG2b combinations, to deposit C4d [42]. These experiments brought us to conclusion that both C1q and MBL participate in complement activation caused by a single subclass of complement-activating antibodies as well as by combinations of complement-activating and non-activating antibodies. Moreover, our findings indicate that while C1q is absolutely required for the synergistic effect of complement activation by a combination of complement-activating and non-complement-activating antibodies, MBL significantly augments this effect.
The role of MBL in organ rejection in humans
A significant percentage of irreversible graft rejections correlate with the presence of high levels of antibodies specific to donor HLA in the circulation and deposition of C4d in the graft.
To date, studies examining the role of MBL in human allograft rejection have been limited and conflicting. Daha’s group found a correlation between higher serum MBL levels and more severe rejections of renal transplants [82, 83]. In kidney allograft biopsies, the presence of C4d was associated with diffuse H-ficolin and IgM deposition in the peritubular capillaries [84] or was colocalized with MBL-associated serine protease 1 (MASP-1) [85]. Our most recent in vitro studies also indicate that anti-HLA antibodies from sera of highly sensitized patients can activate complement through MBL pathway since, in the absence of MBL, C4d deposition on specific target cells is significantly inhibited (70–85%) [86].
To our knowledge, there is only one study documenting increased acute rejection episodes and allograft vasculopathy in MBL-deficient cardiac allograft recipients [87].
The exact mechanism by which MBL binds to a certain combination of complement-activating and non-activating antibodies is the subject of intense investigation. However, in the context of available data, it is possible that the glycosylation patterns of the antibodies used in our studies may be partly responsible for the observed synergistic effects.
Malhotra et al. [81] previously reported that certain circulating IgG molecules in patients with rheumatoid arthritis can activate complement through the MBL pathway. The mechanism of this activation has been attributed to IgG glycoforms known as IgG-G0 glycoforms. IgG-G0 glycoforms lack galactose in ASN297 sugar moiety in the Fc fragment of IgG and terminate in N-acetyl glucosamine (GlcNAc), which allows binding of MBL. In general, development of adaptive immune responses results in the reduction of fully sialylated and galactosylated forms of IgG and the switch from anti- to pro-inflammatory properties of IgG. Patients with high levels of IgG-G0 are more prone to develop autoimmune diseases [88-93]. Our most recent and preliminary studies (unpublished) indicate that in sera from highly sensitized transplant patients, there is a higher level of IgG-G0 glycoforms than in normal individuals.
McMullen et al. [79] have demonstrated that MBL can bind human IgM using surface plasmon resonance and that IgM cause lysis of sensitized red blood cells more effectively in MBL-sufficient sera than MBL-deficient sera. It is important to note that not all IgM antibodies have the ability to activate MBL. This may be attributed to different efficiency to activate complement by hexameric versus pentameric forms of IgM [94, 95]. IgM-induced MBL-dependent complement activation has also been implicated in ischemia reperfusion injury in hearts [79, 96].
Clinically, prospective transplant recipients are screened for potentially harmful antibodies to HLA. Low levels of preformed antibodies detected by flow cytometry alone are considered as “permissible”. However, these antibodies may represent a risk of rejection due to the presence of donor-specific memory B cells [97]. In contrast, antibodies detected by complement-dependent cytotoxicity test (CDC) are “non-permissible”, indicating an unacceptably high risk of graft rejection [1].
While the effects of complement-activating antibodies have been studied extensively, the effects of alloantibodies that do not activate complement are less clear. Titers of non-complement-activating alloantibodies in transplant recipients can be significant in relation to complement-activating alloantibodies [98, 99]. Moreover, their presence can increase the risk for development of early acute rejections after kidney transplantation [100].
In the most recent studies, we demonstrated a significant C4d deposition on specific target cells which were reacted with sera from highly sensitized transplant patients. These sera samples contained low levels of complement-activating antibodies that were dominated by non-complement-activating antibodies. Experiments performed in our laboratory in animal models have also shown that non-complement-activating alloantibodies can be present in higher titers than complement-activating alloantibodies in response to presensitization by blood transfusion [101], as well as in acute rejection of H-2 incompatible mouse cardiac allografts [40, 41].
In vitro models of antibody and complement-mediated endothelial cell injury
Many in vitro studies have demonstrated that antibody and complement have the potential to initiate a dynamic activation of endothelial cells.
Complement is one mediator of antibody-initiated injury that has been demonstrated to promote inflammation by using cultured vascular endothelial cells and purified complement components [54, 55, 67, 68, 102-108]. As an alternative mechanism to complement activation, antibodies have been shown to activate endothelial cells directly in vitro by cross-linking MHC molecules leading to proliferation, increased phosphorylation of tyrosine proteins [109, 110] and production of growth factors or their receptors (TGF-β, PDGF and FGF), MCP-1, cytokines and adhesion molecules [109, 111-115].
In the presence of antibodies, endothelial cells may also acquire resistance to immune-mediated injury known as accommodation [17-19]. Narayanan et al. [116] have shown that exposure of human aortic endothelial cells to saturating concentrations of MHC class I antibodies and complement can induce caspase 3-dependent apoptotic cell death, while sub-saturating concentrations of the same antibodies conferred resistance to antibody and complement-mediated lysis, induced anti-apoptotic genes and anti-inflammatory cytokines [117]. The induction of anti-apoptotic genes has also been demonstrated in models of xenotransplantation [118, 119]. In the presence of low levels of antibodies specific to endothelial or HLA antigens, kidney transplants function well, despite reemergence of donor-specific anti-HLA and/or ABO antibodies. The mechanism of accommodation, although studied intensively, remains to be elucidated.
The role of FcγRs in modulation of immune responses
Receptors for the Fc domain of IgG (FcγR) provide a critical link between specific humoral responses and the cellular pathways of the immune system. Antibodies not only activate complement, but also provide powerful feedback through FcγRs to increase complement production. Likewise, in addition to stimulating production of antibodies by B cells, complement split products can modulate the expression and function of FcR for antibodies. The potential mechanisms by which antibodies can initiate vascular pathology have been examined extensively in vitro [40, 41, 116, 117]. Alloantibodies can direct and augment target cell injury by monocytes, macrophages and NK cells by antibody-dependent cell-mediated cytotoxicity (ADCC) [120-122] and through their Fc receptors [123-125].
To date, four different classes of FcγRs have been identified in mice: the high affinity IgG-FcγRI and three intermediate/low affinity IgG receptors FcγRIIB, FcγRIII and FcγRIV. Functionally, two general classes of FcγRs for IgG are now recognized: (1) the activation receptors FcγRI, FcγRIII and FcγRIV, characterized by the presence of a cytoplasmic ITAM sequence motif associated with the receptor and (2) the inhibitory receptor FcγRIIB characterized by the presence of an immunoreceptor tyrosine-based inhibitory ITIM sequence motif [126-130]. These two classes of receptors function in concert and are usually co-expressed on the cell surface. FcγRI, FcγRIIB and FcγRIV are expressed by variety of lymphoid cell populations: macrophages, monocytes, NK, PMNs and T cells. They mediate effector functions, including phagocytosis, ADCC and the release of inflammatory mediators, whereas FcγRIIB are expressed on both myeloid and lymphoid lineages. Only two types of cells do not co-express activating and inhibitory receptors: NK cells express exclusively FcγRIII, and B cells express inhibitory FcγRIIB [128, 130].
All mouse IgG subclasses can bind to FcγRI, FcγRIII and FcγRIV receptors expressed primarily on cells of the myeloid lineage. FcγRI is constitutively expressed on monocytes and macrophages. Through preferential high affinity binding to IgG2a and IgG2b in mice, FcγRI can induce ADCC [131-133] and may contribute to some graft rejection episodes [122, 134].
Activating FcγRIII interacts preferentially with IgG1. FcγRIII has the highest binding affinity to mouse IgG1 subclass (<107 M−1, Table 1). The affinity of binding of other subclasses is lower (IgG1 > Ig2a > IgG2b) [125, 133]. Cross-linking of FcγRIII, but not FcγRI or FcγRII, on human PBMC induces high levels of MCP-1 [135] and IL-8 [136].
Table 1.
The affinity of binding mouse IgG subclasses to FcγRs
| Receptor | The affinity of binding |
|---|---|
| FcγRI | 107–108 M−1 for IgG2a ≫ IgG1 > IgG2b |
| FcγRIII | <107 M−1 for IgG1 > Ig2a > IgG2b |
| FcγRIV | <107 M−1 for IgG2a > IgG1 > IgG2b |
Activating Fcγ receptors are counter balanced by FcγRIIB on macrophages that functions through an ITIM motif. FcγRIIB is also expressed by B lymphocytes and functions as a feed back inhibitor of antibody production. The balance of activating and inhibitory FcγRs expression by macrophages is controlled by different mediators including cytokines and complement split products.
The role of FcγRs in cardiac allograft transplantation in vivo and in vitro
Antibody interactions with Fcγ and complement receptors on macrophages
Macrophages are a major component of cellular infiltrate in acutely [137] and chronically rejected transplants [27, 138, 139]. In clinical specimens, macrophages and monocytes have been recognized as a correlate of humoral rejection in both renal and cardiac transplants [27, 140, 141]. It is now evident that the initial exposure of macrophages to pro-or anti-inflammatory cytokines determines the function of macrophages and directs them toward inflammatory or reparative functions [142]. Stimulation of macrophages through different Fc receptors modulates their pro- or anti-inflammatory responses [135, 143, 144].
It is well documented that IgG1-mediated injury is associated with the ability of IgG1 to increase interactions with macrophages through FcγRs [125]. Engagement of stimulatory FcγRs, especially FcγRIII by IgG1 causes the accumulation of macrophages in sites of inflammation and blocks their apoptosis [145, 146]. The contribution of FcγRIII to the generation of different pro-inflammatory cytokines and chemokines, such as TNF-α, IL-1-α and MIP-2, has been shown in an experimental model of hypersensitivity pneumonitis/alveolitis in vivo [143]. A dominant role of FcγRIII has been demonstrated in the induction of both TNF-α and IL-1-α production by human macrophages from patients with rheumatoid arthritis [147]. Macrophage production of C3 and C5 is increased through both the Fc [148, 149] and C1q receptors [150]. Gessner et al. [148, 149] have found that production and cleavage of C5 by macrophages is regulated by FcγRs. These researchers have demonstrated a feedback loop between FcγRs and C5a in several models of autoimmunity. In these models, C5 synthesis and cleavage is upregulated by antibodies engaging FcγRIII. Binding of the resulting C5a split product to C5a receptors (C5aR) on macrophages, in turn, upregulates stimulatory FcγRIII and downregulates inhibitory FcγRIIB. This feedback is independent of the early components of complement because it occurs in C3 knockout mice.
The inflammatory effects of alloantibody Fc fragment interaction with Fcγ receptors on mouse endothelial cells (SVEC4-10) cocultured with macrophages in vitro
Our in vitro studies, performed in a model of SVEC4-10 cells sensitized with alloantibodies to MHC class I in the presence of macrophages, indicate that in the absence of complement, IgG1 alloantibodies can cross-link MHC antigens to stimulate endothelial cells to produce MCP-1 and activate macrophages [41]. Consequently, macrophages respond to MCP-1 and produce IL-6. These in vitro findings are of relevance to antibody-mediated rejection in vivo because MCP-1 is a very potent chemotactic protein recruiting neutrophils and monocytes to the site of injury [63, 64]. Our in vitro experiments indicate that FcγRIII expressed on alloantigen-primed macrophages, lymph node or spleen cells is critical to IgG1-mediated activation of endothelial cells. These experiments have shown that the expression of both MCP-1 and IL-6 was severely impaired in cocultures of endothelial cells with macrophages or lymphoid cells from FcγRIII-KO mice [65].
We also found that TNF-α augmented the effects of the IgG1 alloantibodies on MCP-1 and IL-8 gene expression and protein production by cultured endothelial cells. TNF-α is relevant to antibody-mediated rejection in vivo on several levels. First, both the macrophages and T lymphocytes that infiltrate grafts during rejection can produce TNF-α. Second, TNF-α can enhance complement-mediated activation of endothelial cells [68]. Finally, TNF-α has been shown to augment human endothelial cell activation by antibodies to MHC class I antigens in the absence of complement [109, 115].
Effects of F(ab’)2 fragments of alloantibodies on SVEC4-10 cocultured with macrophages in vitro
The importance of FcR interactions with antibodies we further confirmed in experiments using F(ab’)2 fragments of antibodies [65].
The levels of MCP-1 and IL-6 in supernatants from cultures of endothelial cells sensitized with F(ab’)2 fragments of alloantibodies and cocultured with peritoneal macrophages were remarkably lower compared to cultures with the whole molecule of antibody. Moreover, macrophages with blocked FcγRIII also produced lower levels of IL-6 compared to macrophages with unblocked receptors. These in vitro observations correspond with in vivo intra-graft low expression of cytokines in Ig-KO cardiac recipients treated with high doses of F(ab’)2 fragments of complement-activating antibodies [65].
Unexpected inhibitory role of FcγRIII in the experimental mouse model of alloantibody-mediated graft rejection in FcγRIII-KO recipients in vivo
In recent studies, we documented that in the model of B10.A hearts transplanted to C57BL/6 FcγRIII-KO mice, the lack of FcγRIII contributes to accelerated and acute cardiac allograft rejection [151]. B10.A hearts transplanted to C57BL/6 FcγRIII-KO recipients were rejected faster than in WT recipients (7–8 vs. 10–14 days, respectively). The rejection was associated with increased IgG2a and IgG2b alloantibody production, intragraft complement activation and C4d deposition, widespread apoptosis of endothelial cells expressed by the presence of activated Caspase 3, significant increase of IFN-γ and decrease of IL-10 mRNA expression. Our data support strongly the concept that the absence of FcγRIII in vivo contributes to the development of strong pro-inflammatory phenotype and antibody-mediated accelerated cardiac allograft rejection.
This is a novel observation, and the mechanism of this phenomenon needs to be elucidated. There are a few reports in the literature (152-154) indicating that the lack of FcγRIII might contribute to the development of autoimmunity. However, no similar studies have been reported in the model of accelerated cardiac graft rejection in FcγRIII-KO mice. In our ongoing studies, we use this new model to study the mechanism of FcγRIII involvement in modulation of complement- and antibody-mediated cardiac rejection.
Our data along with a body of literature on the role of FcγRs in immune responses indicate that more understanding of FcγR-mediated regulation of macrophage and endothelial cell activation is essential in order to define the role of macrophage infiltrates during antibody-mediated rejection.
In summary, this review describes some of the complex interactions of antibodies, especially their Fc fragments with complement and Fcγ receptors resulting in activation of endothelial cells and macrophages ultimately leading to graft rejection (Fig. 2).
We propose that antibody-mediated injury and graft rejection result from activation of complement by C1q- and MBL-dependent pathways, interaction of complement split products with complement receptors as well as stimulation of IgG-FcγR-dependent interactions. In this model (Fig. 2), alloantibodies bound to endothelial cells initiate complement activation through classical- and MBL-dependent pathways and activate macrophages via complement, complement and Fcγ receptors to produce pro-inflammatory cytokines, IL-1-α, IL-1-β, IL-6 and TNF-α. We believe that oligosaccharides on the Fc fragment of antibody modulate the function of IgG subclasses, especially activation of complement and interaction with Fcγ receptors expressed on mononuclear cells. We also postulate that glycosylation patterns of anti-MHC IgG alloantibodies significantly contribute to the development of pro- or anti-inflammatory immune responses leading to graft injury or protection.
Acknowledgments
The author would like to thank Dr. William M. Baldwin, III for critical review of the manuscript and help with the preparation of Fig. 1, and Dr. Joan Glick Bieler for the help with the editing of the manuscript. The author was supported by grants: NIH R01-HL63948, American Heart Association Grant-in-Aid, Roche Organ Transplantation Research Foundation (ROTRF) grants ID#508303540 and #513443778, Talecris Biotherapeutics, Inc., Talent Program grant.
References
- 1.Patel R, Terasaki PI. Significance of the positive crossmatch test in kidney transplantation. N Engl J Med. 1969;280:735–9. doi: 10.1056/NEJM196904032801401. [DOI] [PubMed] [Google Scholar]
- 2.Feucht HE, Felber E, Gokel MJ, Hillebrand G, Nattermann U, Brockmeyer C, et al. Vascular deposition of complement-split products in kidney allografts with cell-mediated rejection. Clin Exp Immunol. 1991;86:464–70. doi: 10.1111/j.1365-2249.1991.tb02954.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Lederer SR, Schneeberger H, Albert E, Johnson JP, Gruber R, Land W, et al. Early renal graft dysfunction. The role of preformed antibodies to DR-typed lymphoblastoid cell lines. Transplantation. 1996;61:213–9. doi: 10.1097/00007890-199601270-00025. [DOI] [PubMed] [Google Scholar]
- 4.Baldwin WM, III, Pruitt SK, Brauer RB, Daha MR, Sanfilippo F. Complement in organ transplantation: contribution to inflammation, injury and rejection. Transplantation. 1995;59:797–808. [PubMed] [Google Scholar]
- 5.Smith RN, Brousaides N, Grazette L, Saidman S, Semigran M, Disalvo T, et al. C4d deposition in cardiac allografts correlates with alloantibody. J Heart Lung Transpl. 2005;24:1202–10. doi: 10.1016/j.healun.2004.07.021. [DOI] [PubMed] [Google Scholar]
- 6.Smith RN, Kawai T, Boskovic S, Nadazdin O, Sachs DH, Cosimi AB, et al. Chronic antibody mediated rejection of renal allografts: pathological, serological and immunologic features in nonhuman primates. Am J Transpl. 2006;6:1790–8. doi: 10.1111/j.1600-6143.2006.01351.x. [DOI] [PubMed] [Google Scholar]
- 7.Uehara S, Chase CM, Cornell LD, Madsen JC, Russell PS, Colvin RB. Chronic cardiac transplant arteriopathy in mice: relationship of alloantibody, C4d deposition and neointimal fibrosis. Am J Transpl. 2007;7:57–65. doi: 10.1111/j.1600-6143.2006.01599.x. [DOI] [PubMed] [Google Scholar]
- 8.Wehner J, Morrell CN, Reynolds T, Rodriguez ER, Baldwin WM., 3rd Antibody and complement in transplant vasculopathy. Circ Res. 2007;100:191–203. doi: 10.1161/01.RES.0000255032.33661.88. [DOI] [PubMed] [Google Scholar]
- 9.Jordan S. IVIG vs. plasmapheresis for desensitization: which is better? Am J Transpl. 2006;6:1510–1. doi: 10.1111/j.1600-6143.2006.01393.x. [DOI] [PubMed] [Google Scholar]
- 10.Jordan SC, Vo AA, Peng A, Toyoda M, Tyan D. Intravenous gammaglobulin (IVIG): a novel approach to improve transplant rates and outcomes in highly HLA-sensitized patients. Am J Transpl. 2006;6:459–66. doi: 10.1111/j.1600-6143.2005.01214.x. [DOI] [PubMed] [Google Scholar]
- 11.Montgomery RA, Cooper M, Kraus E, Rabb H, Samaniego M, Simpkins CE, et al. Renal transplantation at the Johns Hopkins Comprehensive Transplant Center. Clin Transpl. 2003:199–213. [PubMed] [Google Scholar]
- 12.Montgomery RA, Zachary AA. Transplanting patients with a positive donor-specific crossmatch: a single center’s perspective. Pediatr Transpl. 2004;8:535–42. doi: 10.1111/j.1399-3046.2004.00214.x. [DOI] [PubMed] [Google Scholar]
- 13.Montgomery RA, Zachary AA, Racusen LC, Leffell MS, King KE, Burdick JF, et al. Plasmapheresis and intravenous immune globulin provides effective rescue therapy for refractory humoral rejection and allows kidneys to be successfully transplanted into cross-match-positive recipients. Transplantation. 2000;70:887–95. doi: 10.1097/00007890-200009270-00006. [DOI] [PubMed] [Google Scholar]
- 14.Haas M, Montgomery RA, Segev DL, Rahman MH, Racusen LC, Bagnasco SM, et al. Subclinical acute antibody-mediated rejection in positive crossmatch renal allografts. Am J Transpl. 2007;7:576–85. doi: 10.1111/j.1600-6143.2006.01657.x. [DOI] [PubMed] [Google Scholar]
- 15.Warren DS, Zachary AA, Sonnenday CJ, King KE, Cooper M, Ratner LE, et al. Successful renal transplantation across simultaneous ABO incompatible and positive crossmatch barriers. Am J Transpl. 2004;4:561–8. doi: 10.1111/j.1600-6143.2004.00364.x. [DOI] [PubMed] [Google Scholar]
- 16.Haas M, Rahman MH, Racusen LC, Kraus ES, Bagnasco SM, Segev DL, et al. C4d and C3d staining in biopsies of ABO- and HLA-incompatible renal allografts: correlation with histologic findings. Am J Transpl. 2006;6:1829–40. doi: 10.1111/j.1600-6143.2006.01356.x. [DOI] [PubMed] [Google Scholar]
- 17.Tang AH, Platt JL. Accommodation of grafts: implications for health and disease. Hum Immunol. 2007;68:645–51. doi: 10.1016/j.humimm.2007.04.003. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Platt JL. C4d and the fate of organ allografts. J Am Soc Nephrol. 2002;13:2417–9. doi: 10.1097/01.asn.0000030140.74450.0b. [DOI] [PubMed] [Google Scholar]
- 19.Lynch RJ, Platt JL. Accommodation in organ transplantation. Curr Opin Organ Transpl. 2008;13:165–70. doi: 10.1097/MOT.0b013e3282f6391e. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Feucht HE, Opelz G. The humoral immune response towards HLA class II determinants in renal transplantation. Kidney Int. 1996;50:1464–75. doi: 10.1038/ki.1996.460. [DOI] [PubMed] [Google Scholar]
- 21.Collins AB, Schneeberger EE, Pascual MA, Saidman SL, Williams WW, Tolkoff N, et al. Complement activation in acute humoral renal allograft rejection: diagnostic significance of C4d deposits in peritubular capillaries. J Am Soc Nephrol. 1999;10:2208–14. doi: 10.1681/ASN.V10102208. [DOI] [PubMed] [Google Scholar]
- 22.Racusen LC, Colvin RB, Solez K, Mihatsch MJ, Halloran PF, Campbell PM, et al. Antibody-mediated rejection criteria—an addition to the banff 97 classification of renal allograft rejection. Am J Transpl. 2003;3:708–14. doi: 10.1034/j.1600-6143.2003.00072.x. [DOI] [PubMed] [Google Scholar]
- 23.Feucht HE. Complement C4d in graft capillaries—the missing link in the recognition of humoral alloreactivity. Am J Transpl. 2003;3:646–52. doi: 10.1034/j.1600-6143.2003.00171.x. [DOI] [PubMed] [Google Scholar]
- 24.Mauiyyedi S, Colvin RB. Humoral rejection in kidney transplantation: new concepts in diagnosis and treatment. Curr Opin Nephrol Hypertens. 2002;11:609–18. doi: 10.1097/00041552-200211000-00007. [DOI] [PubMed] [Google Scholar]
- 25.Herzenberg AM, Gill JS, Djurdjev O, Magil AB. C4d deposition in acute rejection: an independent long-term prognostic factor. J Am Soc Nephrol. 2002;13:234–41. doi: 10.1681/ASN.V131234. [DOI] [PubMed] [Google Scholar]
- 26.Lederer SR, Kluth-Pepper B, Schneeberger H, Albert E, Land W, Feucht HE. Impact of humoral alloreactivity early after transplantation on the long-term survival of renal allografts. Kidney Int. 2001;59:334–41. doi: 10.1046/j.1523-1755.2001.00495.x. [DOI] [PubMed] [Google Scholar]
- 27.Michaels PJ, Espejo ML, Kobashigawa J, Alejos JC, Burch C, Takemoto S, et al. Humoral rejection in cardiac transplantation: risk factors, hemodynamic consequences and relationship to transplant coronary artery disease. J Heart Lung Transpl. 2003;22:58–69. doi: 10.1016/s1053-2498(02)00472-2. [DOI] [PubMed] [Google Scholar]
- 28.Mengel M, Bogers J, Bosmans JL, Seron D, Moreso F, Carrera M, et al. Incidence of C4d stain in protocol biopsies from renal allografts: results from a multicenter trial. Am J Transpl. 2005;5:1050–6. doi: 10.1111/j.1600-6143.2005.00788.x. [DOI] [PubMed] [Google Scholar]
- 29.Rodriguez ER, Skojec DV, Tan CD, Zachary AA, Kasper EK, Conte JV, et al. Antibody-mediated rejection in human cardiac allografts: evaluation of immunoglobulins and complement activation products C4d and C3d as markers. Am J Transpl. 2005;5:2778–85. doi: 10.1111/j.1600-6143.2005.01074.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30.Baldwin WM, III, Flavahan NA, Fairchild RL. Integration of complement and leukocytes in response to allotransplantation. Curr Opin Transpl. 2002;7:92–9. [Google Scholar]
- 31.Baldwin WM, III, Larsen CP, Fairchild RL. Innate immune responses to transplants: a significant variable with cadaver donors. Immunity. 2001;14:369–76. doi: 10.1016/s1074-7613(01)00117-0. [DOI] [PubMed] [Google Scholar]
- 32.Sacks SH, Chowdhury P, Zhou W. Role of the complement system in rejection. Curr Opin Immunol. 2003;15:487–92. doi: 10.1016/s0952-7915(03)00100-6. [DOI] [PubMed] [Google Scholar]
- 33.Sacks SH, Zhou W. Locally produced complement and its role in renal allograft rejection. Am J Transpl. 2003;3:927–32. doi: 10.1034/j.1600-6143.2003.00175.x. [DOI] [PubMed] [Google Scholar]
- 34.Qian Z, Wasowska BA, Behrens E, Brody JR, Kadkol SS, Cangello DL, et al. C6 produced by macrophages contributes to cardiac allograft rejection. Am J Pathol. 1999;155:1293–302. doi: 10.1016/S0002-9440(10)65231-5. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 35.Nakashima S, Qian Z, Rahimi S, Wasowska BA, Baldwin WM., 3rd Membrane attack complex contributes to destruction of vascular integrity in acute lung allograft rejection. J Immunol. 2002;169:4620–7. doi: 10.4049/jimmunol.169.8.4620. [DOI] [PubMed] [Google Scholar]
- 36.Nakashima S, Soong TR, Fox-Talbot K, Qian Z, Rahimi S, Wasowska BA, et al. Impact of MHC class II incompatibility on localization of mononuclear cell infiltrates to the bronchiolar compartment of orthotopic lung allografts. Am J Transpl. 2005;5:694–701. doi: 10.1111/j.1600-6143.2005.00782.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 37.Marsh JE, Farmer CK, Jurcevic S, Wang Y, Carroll MC, Sacks SH. The allogeneic T and B cell response is strongly dependent on complement components C3 and C4. Transplantation. 2001;72:1310–8. doi: 10.1097/00007890-200110150-00022. [DOI] [PubMed] [Google Scholar]
- 38.Pratt JR, Basheer SA, Sacks SH. Local synthesis of complement component C3 regulates acute renal transplant rejection. Nat Med. 2002;8:582–7. doi: 10.1038/nm0602-582. [DOI] [PubMed] [Google Scholar]
- 39.Li K, Patel H, Farrar CA, Hargreaves RE, Sacks SH, Zhou W. Complement regulates the capacity of proximal tubular epithelial cell to stimulate alloreactive T cell response. J Am Soc Nephrol. 2004;15:2414–22. doi: 10.1097/01.ASN.0000135974.06478.7B. [DOI] [PubMed] [Google Scholar]
- 40.Wasowska BA, Qian Z, Cangello DL, Behrens E, Van Tran K, Layton J, et al. Passive transfer of alloantibodies restores acute cardiac rejection in IgKO mice. Transplantation. 2001;71:727–36. doi: 10.1097/00007890-200103270-00007. [DOI] [PubMed] [Google Scholar]
- 41.Rahimi S, Qian Z, Layton J, Fox-Talbot K, Baldwin WM, Wasowska BA. Non-complement and complement activating antibodies synergize to cause rejection of cardiac allografts. Am J Transpl. 2004;4:326–34. doi: 10.1111/j.1600-6143.2004.00334.x. [DOI] [PubMed] [Google Scholar]
- 42.Murata K, Fox-Talbot K, Qian Z, Takahashi K, Stahl GL, Baldwin WM, Wasowska BA. Synergistic deposition of C4d by complement-activating and non-activating antibodies in cardiac transplants. Am J Transpl. 2007;7:2605–14. doi: 10.1111/j.1600-6143.2007.01971.x. [DOI] [PubMed] [Google Scholar]
- 43.Brandle D, Joergensen J, Zenke G, Burki K, Hof RP. Contribution of donor-specific antibodies to acute allograft rejection: evidence from B cell-deficient mice. Transplantation. 1998;65:1489–93. doi: 10.1097/00007890-199806150-00014. [DOI] [PubMed] [Google Scholar]
- 44.Jindra PT, Hsueh A, Hong L, Gjertson D, Shen XD, Gao F, et al. Anti-MHC class I antibody activation of proliferation and survival signaling in murine cardiac allografts. J Immunol. 2008;180:2214–24. doi: 10.4049/jimmunol.180.4.2214. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 45.Wasowska BA, Qian Z, Behrens E, Cangello D, Sanfilippo F, Baldwin WM., III Inhibition of acute cardiac allograft rejection in immunoglobulin-deficient mice. Transpl Proc. 1999;31:136. doi: 10.1016/s0041-1345(98)01476-6. [DOI] [PubMed] [Google Scholar]
- 46.Salomon B, Bluestone JA. Complexities of CD28/B7: CTLA-4 costimulatory pathways in autoimmunity and transplantation. Annu Rev Immunol. 2001;19:225–52. doi: 10.1146/annurev.immunol.19.1.225. [DOI] [PubMed] [Google Scholar]
- 47.Reed EF, Demetris AJ, Hammond E, Itescu S, Kobashigawa JA, Reinsmoen NL, et al. Acute antibody-mediated rejection of cardiac transplants. J Heart Lung Transpl. 2006;25:153–9. doi: 10.1016/j.healun.2005.09.003. [DOI] [PubMed] [Google Scholar]
- 48.Meehan SM, Limsrichamrern S, Manaligod JR, Junsanto T, Josephson MA, Thistlethwaite JR. Platelets and capillary injury in acute humoral rejection of renal allografts. Hum Pathol. 2003;34:533–40. doi: 10.1016/s0046-8177(03)00189-8. [DOI] [PubMed] [Google Scholar]
- 49.Morrell CN, Murata K, Swaim AM, Mason E, Martin TV, Thompson LE, et al. In vivo platelet-endothelial cell interactions in response to major histocompatibility complex alloantibody. Circ Res. 2008;102:777–85. doi: 10.1161/CIRCRESAHA.107.170332. [DOI] [PubMed] [Google Scholar]
- 50.Ota H, Fox-Talbot K, Hu W, Qian Z, Sanfilippo F, Hruban RH, et al. Terminal complement components mediate release of von Willebrand factor and adhesion of platelets in arteries of allografts. Transplantation. 2005;79:276–81. doi: 10.1097/01.tp.0000146195.76904.d3. [DOI] [PubMed] [Google Scholar]
- 51.Morrell CN, Sun H, Swaim AM, Baldwin WM., 3rd Platelets an inflammatory force in transplantation. Am J Transpl. 2007;7:2447–54. doi: 10.1111/j.1600-6143.2007.01958.x. [DOI] [PubMed] [Google Scholar]
- 52.Kirk AD, Morrell CN, Baldwin WM., 3rd Platelets influence vascularized organ transplants from start to finish. Am J Transpl. 2009;9:14–22. doi: 10.1111/j.1600-6143.2008.02473.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 53.Saadi S, Holzknecht RA, Patte CP, Platt JL. Endothelial cell activation by pore-forming structures: pivotal role for interleukin-1alpha. Circulation. 2000;101:1867–73. doi: 10.1161/01.cir.101.15.1867. [DOI] [PubMed] [Google Scholar]
- 54.Saadi S, Holzknecht RA, Patte CP, Stern DM, Platt JL. Complement-mediated regulation of tissue factor activity in endothelium. J Exp Med. 1995;182:1807–14. doi: 10.1084/jem.182.6.1807. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 55.Tedesco F, Pausa M, Nardon E, Introna M, Mantovani A, Dobrina A. The cytolytically inactive terminal complement complex activates endothelial cells to express adhesion molecules and tissue factor procoagulant activity. J Exp Med. 1997;185:1619–27. doi: 10.1084/jem.185.9.1619. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 56.Schulte am Esch J, II, Cruz MA, Siegel JB, Anrather J, Robson SC. Activation of human platelets by the membrane-expressed A1 domain of von Willebrand factor. Blood. 1997;90:4425–37. [PubMed] [Google Scholar]
- 57.Bombeli T, Schwartz BR, Harlan JM. Adhesion of activated platelets to endothelial cells: evidence for a GPIIbIIIa-dependent bridging mechanism and novel roles for endothelial intercellular adhesion molecule 1 (ICAM-1), alphavbeta3 integrin, and GPIbalpha. J Exp Med. 1998;187:329–39. doi: 10.1084/jem.187.3.329. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 58.Yamakuchi M, Kirkiles-Smith NC, Ferlito M, Cameron SJ, Bao C, Fox-Talbot K, et al. Antibody to human leukocyte antigen triggers endothelial exocytosis. Proc Natl Acad Sci USA. 2007;104:1301–6. doi: 10.1073/pnas.0602035104. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 59.Lowenstein CJ, Morrell CN, Yamakuchi M. Regulation of Weibel-Palade body exocytosis. Trends Cardiovasc Med. 2005;15:302–8. doi: 10.1016/j.tcm.2005.09.005. [DOI] [PubMed] [Google Scholar]
- 60.Celi A, Pellegrini G, Lorenzet R, De Blasi A, Ready N, Furie BC, et al. P-selectin induces the expression of tissue factor on monocytes. Proc Natl Acad Sci USA. 1994;91:8767–71. doi: 10.1073/pnas.91.19.8767. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 61.Weyrich AS, McIntyre TM, McEver RP, Prescott SM, Zimmerman GA. Monocyte tethering by P-selectin regulates monocyte chemotactic protein-1 and tumor necrosis factor-alpha secretion. Signal integration and NF-kappa B translocation. J Clin Investig. 1995;95:2297–303. doi: 10.1172/JCI117921. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 62.Weyrich AS, Elstad MR, McEver RP, McIntyre TM, Moore KL, Morrissey JH, et al. Activated platelets signal chemokine synthesis by human monocytes. J Clin Investig. 1996;97:1525–34. doi: 10.1172/JCI118575. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 63.Kilgore KS, Schmid E, Shanley TP, Flory CM, Maheswari V, Tramontini NL, et al. Sublytic concentrations of the membrane attack complex of complement induce endothelial interleukin-8 and monocyte chemoattractant protein-1 through nuclear factor-kappa B activation. Am J Pathol. 1997;150:2019–31. [PMC free article] [PubMed] [Google Scholar]
- 64.Torzewski J, Oldroyd R, Lachmann P, Fitzsimmons C, Proudfoot D, Bowyer D. Complement-induced release of monocyte chemotactic protein-1 from human smooth muscle cells. A possible initiating event in atherosclerotic lesion formation. Arterioscler Thromb Vasc Biol. 1996;16:673–7. doi: 10.1161/01.atv.16.5.673. [DOI] [PubMed] [Google Scholar]
- 65.Lee C-Y, Lotfi-Emran S, Erdinc M, Murata K, Velidedeoglu E, Fox-Talbot K, et al. The involvement of FcR mechanisms in antibody-mediated rejection. Transplantation. 2007;9:33–43. doi: 10.1097/01.tp.0000287457.54761.53. [DOI] [PubMed] [Google Scholar]
- 66.Qian Z, Jakobs FM, Pfaff-Amesse T, Sanfilippo F, Baldwin WM., 3rd Complement contributes to the rejection of complete and class I major histocompatibility complex–incompatible cardiac allografts. J Heart Lung Transpl. 1998;17:470–8. [PubMed] [Google Scholar]
- 67.Hattori R, Hamilton KK, McEver RP, Sims PJ. Complement proteins C5b–C9 induce secretion of high molecular weight multimers of endothelial von Willebrand factor and translocation of granule membrane protein GMP-140 to the cell surface. J Biol Chem. 1989;264:9053–60. [PubMed] [Google Scholar]
- 68.Kilgore KS, Shen JP, Miller BF, Ward PA, Warren JS. Enhancement by the complement membrane attack complex of tumor necrosis factor-alpha-induced endothelial cell expression of E-selectin and ICAM-1. J Immunol. 1995;155:1434–41. [PubMed] [Google Scholar]
- 69.Selvan RS, Kapadia HB, Platt JL. Complement-induced expression of chemokine genes in endothelium: regulation by IL-1-dependent and -independent mechanisms. J Immunol. 1998;161:4388–95. [PubMed] [Google Scholar]
- 70.Hawrylowicz CM, Howells GL, Feldmann M. Platelet-derived interleukin 1 induces human endothelial adhesion molecule expression and cytokine production. J Exp Med. 1991;174:785–90. doi: 10.1084/jem.174.4.785. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 71.Soslau G, Morgan DA, Jaffe JS, Brodsky I, Wang Y. Cytokine mRNA expression in human platelets and a megakaryocytic cell line and cytokine modulation of platelet function. Cytokine. 1997;9:405–11. doi: 10.1006/cyto.1996.0182. [DOI] [PubMed] [Google Scholar]
- 72.Ey PL, Prowse SJ, Jenkin CR. Complement-fixing IgG1 constitutes a new subclass of mouse IgG. Nature. 1979;281:492–3. doi: 10.1038/281492a0. [DOI] [PubMed] [Google Scholar]
- 73.Ey PL, Russell-Jones GJ, Jenkin CR. Isotypes of mouse IgG–I. Evidence for ‘non-complement-fixing’ IgG1 antibodies and characterization of their capacity to interfere with IgG2 sensitization of target red blood cells for lysis by complement. Mol Immunol. 1980;17:699–710. doi: 10.1016/0161-5890(80)90139-x. [DOI] [PubMed] [Google Scholar]
- 74.Neuberger MS, Rajewsky K. Activation of mouse complement by monoclonal mouse antibodies. Eur J Immunol. 1981;11:1012–6. doi: 10.1002/eji.1830111212. [DOI] [PubMed] [Google Scholar]
- 75.White KD, Frank MB, Foundling S, Waxman FJ. Effect of immunoglobulin variable region structure on C3b and C4b deposition. Mol Immunol. 1996;33:759–68. doi: 10.1016/0161-5890(96)00031-4. [DOI] [PubMed] [Google Scholar]
- 76.Yokoyama I, Waxman F. Differential susceptibility of immune complexes to release from the erythrocyte CR1 receptor by factor I. Mol Immunol. 1994;31:227–40. doi: 10.1016/0161-5890(94)90003-5. [DOI] [PubMed] [Google Scholar]
- 77.Bindon CI, Hale G, Waldmann H. Importance of antigen specificity for complement-mediated lysis by monoclonal antibodies. Eur J Immunol. 1988;18:1507–14. doi: 10.1002/eji.1830181006. [DOI] [PubMed] [Google Scholar]
- 78.Dommett RM, Klein N, Turner MW. Mannose-binding lectin in innate immunity: past, present and future. Tissue Antigens. 2006;68:193–209. doi: 10.1111/j.1399-0039.2006.00649.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 79.McMullen ME, Hart ML, Walsh MC, Buras J, Takahashi K, Stahl GL. Mannose-binding lectin binds IgM to activate the lectin complement pathway in vitro and in vivo. Immunobiology. 2006;211:759–66. doi: 10.1016/j.imbio.2006.06.011. [DOI] [PubMed] [Google Scholar]
- 80.Chan RK, Ibrahim SI, Takahashi K, Kwon E, McCormack M, Ezekowitz A, et al. The differing roles of the classical and mannose-binding lectin complement pathways in the events following skeletal muscle ischemia-reperfusion. J Immunol. 2006;177:8080–5. doi: 10.4049/jimmunol.177.11.8080. [DOI] [PubMed] [Google Scholar]
- 81.Malhotra R, Wormald MR, Rudd PM, Fischer PB, Dwek RA, Sim RB. Glycosylation changes of IgG associated with rheumatoid arthritis can activate complement via the mannose-binding protein. Nat Med. 1995;1:237–43. doi: 10.1038/nm0395-237. [DOI] [PubMed] [Google Scholar]
- 82.Berger SP, Roos A, Mallat MJ, Fujita T, de Fijter JW, Daha MR. Association between mannose-binding lectin levels and graft survival in kidney transplantation. Am J Transpl. 2005;5:1361–6. doi: 10.1111/j.1600-6143.2005.00841.x. [DOI] [PubMed] [Google Scholar]
- 83.Berger SP, Roos A, Mallat MJ, Schaapherder AF, Doxiadis II, van Kooten C, et al. Low pretransplantation mannose-binding lectin levels predict superior patient and graft survival after simultaneous pancreas-kidney transplantation. J Am Soc Nephrol. 2007;18:2416–22. doi: 10.1681/ASN.2007030262. [DOI] [PubMed] [Google Scholar]
- 84.Imai N, Nishi S, Alchi B, Ueno M, Fukase S, Arakawa M, et al. Immunohistochemical evidence of activated lectin pathway in kidney allografts with peritubular capillary C4d deposition. Nephrol Dial Transpl. 2006;21:2589–95. doi: 10.1093/ndt/gfl210. [DOI] [PubMed] [Google Scholar]
- 85.Sund S, Hovig T, Reisaeter AV, Scott H, Bentdal O, Mollnes TE. Complement activation in early protocol kidney graft biopsies after living-donor transplantation. Transplantation. 2003;75:1204–13. doi: 10.1097/01.TP.0000062835.30165.2C. [DOI] [PubMed] [Google Scholar]
- 86.Erdinc M, Mcgregor A, Lucas DP, Leffell MS, Montgomery RA, Zachary AA, et al. IVIg inhibits C1q- and mannose binding lectin (MBL)-dependent deposition of C4d by human alloantibodies. Am J Transpl. 2008;8(s2):568. [Google Scholar]
- 87.Fiane AE, Ueland T, Simonsen S, Scott H, Endresen K, Gullestad L, et al. Low mannose-binding lectin and increased complement activation correlate to allograft vasculopathy, ischaemia, and rejection after human heart transplantation. Eur Heart J. 2005;26:1660–5. doi: 10.1093/eurheartj/ehi198. [DOI] [PubMed] [Google Scholar]
- 88.Arnold JN, Wormald MR, Sim RB, Rudd PM, Dwek RA. The impact of glycosylation on the biological function and structure of human immunoglobulins. Annu Rev Immunol. 2007;25:21–50. doi: 10.1146/annurev.immunol.25.022106.141702. [DOI] [PubMed] [Google Scholar]
- 89.Garred P, Madsen HO, Marquart H, Hansen TM, Sorensen SF, Petersen J, et al. Two edged role of mannose binding lectin in rheumatoid arthritis: a cross sectional study. J Rheumatol. 2000;27:26–34. [PubMed] [Google Scholar]
- 90.Rademacher TW, Williams P, Dwek RA. Agalactosyl glycoforms of IgG autoantibodies are pathogenic. Proc Natl Acad Sci USA. 1994;91:6123–7. doi: 10.1073/pnas.91.13.6123. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 91.Bond A, Alavi A, Axford JS, Bourke BE, Bruckner FE, Kerr MA, et al. A detailed lectin analysis of IgG glycosylation, demonstrating disease specific changes in terminal galactose and N-acetylglucosamine. J Autoimmun. 1997;10:77–85. doi: 10.1006/jaut.1996.0104. [DOI] [PubMed] [Google Scholar]
- 92.Rook GA, Steele J, Brealey R, Whyte A, Isenberg D, Sumar N, et al. Changes in IgG glycoform levels are associated with remission of arthritis during pregnancy. J Autoimmun. 1991;4:779–94. doi: 10.1016/0896-8411(91)90173-a. [DOI] [PubMed] [Google Scholar]
- 93.Parekh RB, Dwek RA, Sutton BJ, Fernandes DL, Leung A, Stanworth D, et al. Association of rheumatoid arthritis and primary osteoarthritis with changes in the glycosylation pattern of total serum IgG. Nature. 1985;316:452–7. doi: 10.1038/316452a0. [DOI] [PubMed] [Google Scholar]
- 94.Collins C, Tsui FW, Shulman MJ. Differential activation of human and guinea pig complement by pentameric and hexameric IgM. Eur J Immunol. 2002;32:1802–10. doi: 10.1002/1521-4141(200206)32:6<1802::AID-IMMU1802>3.0.CO;2-C. [DOI] [PubMed] [Google Scholar]
- 95.Arnold JN, Wormald MR, Suter DM, Radcliffe CM, Harvey DJ, Dwek RA, et al. Human serum IgM glycosylation: identification of glycoforms that can bind to mannan-binding lectin. J Biol Chem. 2005;280:29080–7. doi: 10.1074/jbc.M504528200. [DOI] [PubMed] [Google Scholar]
- 96.Walsh MC, Bourcier T, Takahashi K, Shi L, Busche MN, Rother RP, et al. Mannose-binding lectin is a regulator of inflammation that accompanies myocardial ischemia and reperfusion injury. J Immunol. 2005;175:541–6. doi: 10.4049/jimmunol.175.1.541. [DOI] [PubMed] [Google Scholar]
- 97.Scornik JC, Clapp W, Patton PR, Van der Werf WJ, Hemming AW, Reed AI, et al. Outcome of kidney transplants in patients known to be flow cytometry crossmatch positive. Transplantation. 2001;71:1098–102. doi: 10.1097/00007890-200104270-00015. [DOI] [PubMed] [Google Scholar]
- 98.Arnold ML, Zacher T, Dechant M, Kalden JR, Doxiadis II, Spriewald BM. Detection and specification of noncomplement binding anti-HLA alloantibodies. Hum Immunol. 2004;65:1288–96. doi: 10.1016/j.humimm.2004.08.182. [DOI] [PubMed] [Google Scholar]
- 99.Kushihata F, Watanabe J, Mulder A, Claas F, Scornik JC. Human leukocyte antigen antibodies and human complement activation: role of IgG subclass, specificity, and cytotoxic potential. Transplantation. 2004;78:995–1001. doi: 10.1097/01.tp.0000136966.63957.e2. [DOI] [PubMed] [Google Scholar]
- 100.Karuppan SS, Ohlman S, Moller E. The occurrence of cytotoxic and non-complement-fixing antibodies in the crossmatch serum of patients with early acute rejection episodes. Transplantation. 1992;54:839–44. doi: 10.1097/00007890-199211000-00014. [DOI] [PubMed] [Google Scholar]
- 101.Qian Z, Lee C, Murata K, Liu J, Fox-Talbot K, Wasowska B, et al. Antibody and complement mediated injury in transplants following sensitization by allogeneic blood transfusion. Transplantation. 2006;2006:857–64. doi: 10.1097/01.tp.0000232335.06792.35. [DOI] [PubMed] [Google Scholar]
- 102.Benzaquen LR, Nicholson-Weller A, Halperin JA. Terminal complement proteins C5b-9 release basic fibroblast growth factor and platelet-derived growth factor from endothelial cells. J Exp Med. 1994;179:985–92. doi: 10.1084/jem.179.3.985. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 103.Kilgore KS, Flory CM, Miller BF, Evans VM, Warren JS. The membrane attack complex of complement induces interleukin-8 and monocyte chemoattractant protein-1 secretion from human umbilical vein endothelial cells. Am J Pathol. 1996;149:953–61. [PMC free article] [PubMed] [Google Scholar]
- 104.Rus HG, Niculescu FI, Shin M. Role of the C5b-9 complement complex in cell cycle and apoptosis. Immunol Rev. 2001;180:49–55. doi: 10.1034/j.1600-065x.2001.1800104.x. [DOI] [PubMed] [Google Scholar]
- 105.DiScipio RG, Daffern PJ, Jagels MA, Broide DH, Sriramarao P. A comparison of C3a and C5a-mediated stable adhesion of rolling eosinophils in postcapillary venules and transendothelial migration in vitro and in vivo. J Immunol. 1999;162:1127–36. [PubMed] [Google Scholar]
- 106.Nataf S, Davoust N, Ames RS, Barnum SR. Human T cells express the C5a receptor and are chemoattracted to C5a. J Immunol. 1999;162:4018–23. [PubMed] [Google Scholar]
- 107.Schraufstatter IU, Trieu K, Sikora L, Sriramarao P, DiScipio R. Complement c3a and c5a induce different signal transduction cascades in endothelial cells. J Immunol. 2002;169:2102–10. doi: 10.4049/jimmunol.169.4.2102. [DOI] [PubMed] [Google Scholar]
- 108.Laudes IJ, Chu JC, Huber-Lang M, Guo RF, Riedemann NC, Sarma JV, et al. Expression and function of C5a receptor in mouse microvascular endothelial cells. J Immunol. 2002;169:5962–70. doi: 10.4049/jimmunol.169.10.5962. [DOI] [PubMed] [Google Scholar]
- 109.Bian H, Reed EF. Alloantibody-mediated class I signal transduction in endothelial cells and smooth muscle cells: enhancement by IFN-gamma and TNF-alpha. J Immunol. 1999;163:1010–8. [PubMed] [Google Scholar]
- 110.Reznik SI, Jaramillo A, Zhang L, Patterson GA, Cooper JD, Mohanakumar T. Anti-HLA antibody binding to hla class I molecules induces proliferation of airway epithelial cells: a potential mechanism for bronchiolitis obliterans syndrome. J Thorac Cardiovasc Surg. 2000;119:39–45. doi: 10.1016/s0022-5223(00)70215-7. [DOI] [PubMed] [Google Scholar]
- 111.Millan MT, Geczy C, Stuhlmeier KM, Goodman DJ, Ferran C, Bach FH. Human monocytes activate porcine endothelial cells, resulting in increased E-selectin, interleukin-8, monocyte chemotactic protein-1, and plasminogen activator inhibitor-type-1 expression. Transplantation. 1997;63:421–9. doi: 10.1097/00007890-199702150-00016. [DOI] [PubMed] [Google Scholar]
- 112.Vos IH, Briscoe DM. Endothelial injury: cause and effect of alloimmune inflammation. Transpl Infect Dis. 2002;4:152–9. doi: 10.1034/j.1399-3062.2002.t01-1-02002.x. [DOI] [PubMed] [Google Scholar]
- 113.Pidwell DJ, Heller MJ, Gabler D, Orosz CG. In vitro stimulation of human endothelial cells by sera from a subpopulation of high-percentage panel-reactive antibody patients. Transplantation. 1995;60:563–9. doi: 10.1097/00007890-199509270-00008. [DOI] [PubMed] [Google Scholar]
- 114.Fredrich R, Toyoda M, Czer LS, Galfayan K, Galera O, Trento A, et al. The clinical significance of antibodies to human vascular endothelial cells after cardiac transplantation. Transplantation. 1999;67:385–91. doi: 10.1097/00007890-199902150-00008. [DOI] [PubMed] [Google Scholar]
- 115.Harris PE, Bian H, Reed EF. Induction of high affinity fibroblast growth factor receptor expression and proliferation in human endothelial cells by anti-HLA antibodies: a possible mechanism for transplant atherosclerosis. J Immunol. 1997;159:5697–704. [PubMed] [Google Scholar]
- 116.Narayanan K, Jendrisak MD, Phelan DL, Mohanakumar T. HLA class I antibody mediated accommodation of endothelial cells via the activation of PI3K/cAMP dependent PKA pathway. Transpl Immunol. 2006;15:187–97. doi: 10.1016/j.trim.2005.09.005. [DOI] [PubMed] [Google Scholar]
- 117.Narayanan K, Naziruddin B, Phelan D, Mohanakumar T. Mechanism for in vitro “accommodation” of human aortic endothelial cells by alloantibodies specific for HLA molecules: down regulation of adhesion molecules and over expression of protective genes. Hum Immunol. 2002;63(10 Suppl):S19. [Google Scholar]
- 118.Soares MP, Lin Y, Anrather J, Csizmadia E, Takigami K, Sato K, et al. Expression of heme oxygenase-1 can determine cardiac xenograft survival. Nat Med. 1998;4:1073–7. doi: 10.1038/2063. [DOI] [PubMed] [Google Scholar]
- 119.Soares MP, Seldon MP, Gregoire IP, Vassilevskaia T, Berberat PO, Yu J, et al. Heme oxygenase-1 modulates the expression of adhesion molecules associated with endothelial cell activation. J Immunol. 2004;172:3553–63. doi: 10.4049/jimmunol.172.6.3553. [DOI] [PubMed] [Google Scholar]
- 120.Abdullah N, Greenman J, Pimendiou A, Topping KP, Monson JR. The role of monocytes and natural killer cells in mediating antibody-dependent lysis of colorectal tumor cells. Cancer Immunol Immunother. 1999;48:517–24. doi: 10.1007/s002620050600. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 121.Macdermott RP, Nash GS, Merkle NS, Weinrieb IJ, Bertovich MJ, Formeister JF. Further evidence that antibody-dependent and spontaneous cell-mediated cytotoxicity are mediated by different processes or cell types. Immunology. 1980;41:439–47. [PMC free article] [PubMed] [Google Scholar]
- 122.Miltenburg AMM, Meijer-Paape ME, Weening JJ, Daha MR, van Es LA, van der Woude FJ. Induction of antibody-dependent cellular cytotoxicity against endothelial cells by renal transplantation. Transplantation. 1989;48:681. [PubMed] [Google Scholar]
- 123.van de Winkel JG, Capel PJ. Human IgG Fc receptor heterogeneity: molecular aspects and clinical implications. Immunol Today. 1993;14:215–21. doi: 10.1016/0167-5699(93)90166-I. [DOI] [PubMed] [Google Scholar]
- 124.Schmidt RE, Gessner JE. Fc receptors and their interaction with complement in autoimmunity. Immunol Lett. 2005;100:56–67. doi: 10.1016/j.imlet.2005.06.022. [DOI] [PubMed] [Google Scholar]
- 125.Ravetch JV, Bolland S. IgG Fc receptors. Annu Rev Immunol. 2001;19:275–90. doi: 10.1146/annurev.immunol.19.1.275. [DOI] [PubMed] [Google Scholar]
- 126.Daeron M. Fc receptor biology. Annu Rev Immunol. 1997;15:203–34. doi: 10.1146/annurev.immunol.15.1.203. [DOI] [PubMed] [Google Scholar]
- 127.Bolland S, Ravetch JV. Inhibitory pathways triggered by ITIM-containing receptors. Adv Immunol. 1999;72:149–77. doi: 10.1016/s0065-2776(08)60019-x. [DOI] [PubMed] [Google Scholar]
- 128.Nimmerjahn F, Ravetch JV. Fc-receptors as regulators of immunity. Adv Immunol. 2007;96:179–204. doi: 10.1016/S0065-2776(07)96005-8. [DOI] [PubMed] [Google Scholar]
- 129.Nimmerjahn F, Bruhns P, Horiuchi K, Ravetch JV. FcgammaRIV: a novel FcR with distinct IgG subclass specificity. Immunity. 2005;23:41–51. doi: 10.1016/j.immuni.2005.05.010. [DOI] [PubMed] [Google Scholar]
- 130.Nimmerjahn F, Ravetch JV. Fcgamma receptors as regulators of immune responses. Nat Rev Immunol. 2008;8:34–47. doi: 10.1038/nri2206. [DOI] [PubMed] [Google Scholar]
- 131.Boot JHA, Geerts MEJ, Aarden LA. Functional polymorphisms of Fc receptor in human monocyte-mediated cytotoxicity towards erythrocytes induced by murine isotype switch variants. J Immunol. 1989;142:1217. [PubMed] [Google Scholar]
- 132.Ravetch JV, Kinet JP. Fc receptors. Annu Rev Immunol. 1991;9:457–92. doi: 10.1146/annurev.iy.09.040191.002325. [DOI] [PubMed] [Google Scholar]
- 133.Dijstelbloem HM, van de Winkel JG, Kallenberg CG. Inflammation in immunity: receptors for IgG revisited. Trends Immunol. 2001;22:510–6. doi: 10.1016/s1471-4906(01)02014-2. [DOI] [PubMed] [Google Scholar]
- 134.Kirby JA, Givan AL, Shenton BK, Talbot D, Forsythe JL, Lennard TW, et al. Renal allograft rejection. Possible involvement of antibody-dependent cell-mediated cytotoxicity. Transplantation. 1990;50:225–9. doi: 10.1097/00007890-199008000-00010. [DOI] [PubMed] [Google Scholar]
- 135.Marsh CB, Wewers MD, Tan LC, Rovin BH. Fc(gamma) receptor cross-linking induces peripheral blood mononuclear cell monocyte chemoattractant protein-1 expression: role of lymphocyte Fc(gamma)RIII. J Immunol. 1997;158:1078–84. [PubMed] [Google Scholar]
- 136.Marsh CB, Gadek JE, Kindt GC, Moore SA, Wewers MD. Monocyte Fc gamma receptor cross-linking induces IL-8 production. J Immunol. 1995;155:3161–7. [PubMed] [Google Scholar]
- 137.Sekine Y, Yasufuku K, Heidler KM, Cummings OW, Van Rooijen N, Fujisawa T, et al. Monocyte chemoattractant protein-1 and RANTES are chemotactic for graft infiltrating lymphocytes during acute lung allograft rejection. Am J Respir Cell Mol Biol. 2000;23:719–26. doi: 10.1165/ajrcmb.23.6.3825. [DOI] [PubMed] [Google Scholar]
- 138.Nadeau KC, Azuma H, Tilney NL. Sequential cytokine expression in renal allografts in rats immunosuppressed with maintenance cyclosporine or mycophenolate mofetil. Transplantation. 1996;62:1363–6. doi: 10.1097/00007890-199611150-00034. [DOI] [PubMed] [Google Scholar]
- 139.Russell ME, Wallace AF, Hancock WW, Sayegh MH, Adams DH, Sibinga NE, et al. Upregulation of cytokines associated with macrophage activation in the Lewis-to-F344 rat transplantation model of chronic cardiac rejection. Transplantation. 1995;59:572–8. [PubMed] [Google Scholar]
- 140.Lones MA, Czer LS, Trento A, Harasty D, Miller JM, Fishbein MC. Clinical-pathologic features of humoral rejection in cardiac allografts: a study in 81 consecutive patients. J Heart Lung Transpl. 1995;14:151–62. [PubMed] [Google Scholar]
- 141.Magil AB, Tinckam K. Monocytes and peritubular capillary C4d deposition in acute renal allograft rejection. Kidney Int. 2003;63:1888–93. doi: 10.1046/j.1523-1755.2003.00921.x. [DOI] [PubMed] [Google Scholar]
- 142.Erwig LP, Kluth DC, Walsh GM, Rees AJ. Initial cytokine exposure determines function of macrophages and renders them unresponsive to other cytokines. J Immunol. 1998;161:1983–8. [PubMed] [Google Scholar]
- 143.Chouchakova N, Skokowa J, Baumann U, Tschernig T, Philippens KM, Nieswandt B, et al. Fc gamma RIII-mediated production of TNF-alpha induces immune complex alveolitis independently of CXC chemokine generation. J Immunol. 2001;166:5193–200. doi: 10.4049/jimmunol.166.8.5193. [DOI] [PubMed] [Google Scholar]
- 144.Latour S, Bonnerot C, Fridman WH, Daeron M. Induction of tumor necrosis factor-alpha production by mast cells via Fc gamma R. Role of the Fc gamma RIII gamma subunit. J Immunol. 1992;149:2155–62. [PubMed] [Google Scholar]
- 145.Wang ZQ, Bapat AS, Rayanade RJ, Dagtas AS, Hoffmann MK. Interleukin-10 induces macrophage apoptosis and expression of CD16 (FcgammaRIII) whose engagement blocks the cell death programme and facilitates differentiation. Immunology. 2001;102:331–7. doi: 10.1046/j.1365-2567.2001.01171.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 146.Coxon A, Cullere X, Knight S, Sethi S, Wakelin MW, Stavrakis G, et al. Fc gamma RIII mediates neutrophil recruitment to immune complexes. A mechanism for neutrophil accumulation in immune-mediated inflammation. Immunity. 2001;14:693–704. doi: 10.1016/s1074-7613(01)00150-9. [DOI] [PubMed] [Google Scholar]
- 147.Abrahams VM, Cambridge G, Lydyard PM, Edwards JC. Induction of tumor necrosis factor alpha production by adhered human monocytes: a key role for Fcgamma receptor type IIIa in rheumatoid arthritis. Arthritis Rheum. 2000;43:608–16. doi: 10.1002/1529-0131(200003)43:3<608::AID-ANR18>3.0.CO;2-G. [DOI] [PubMed] [Google Scholar]
- 148.Shushakova N, Skokowa J, Schulman J, Baumann U, Zwirner J, Schmidt RE, et al. C5a anaphylatoxin is a major regulator of activating versus inhibitory FcgammaRs in immune complex-induced lung disease. J Clin Investig. 2002;110:1823–30. doi: 10.1172/JCI200216577. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 149.Kumar V, Ali SR, Konrad S, Zwirner J, Verbeek JS, Schmidt RE, et al. Cell-derived anaphylatoxins as key mediators of antibody-dependent type II autoimmunity in mice. J Clin Investig. 2006;116:512–20. doi: 10.1172/JCI25536. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 150.Bajtay Z, Jozsi M, Banki Z, Thiel S, Thielens N, Erdei A. Mannan-binding lectin and C1q bind to distinct structures and exert differential effects on macrophages. Eur J Immunol. 2000;30:1706–13. doi: 10.1002/1521-4141(200006)30:6<1706::AID-IMMU1706>3.0.CO;2-2. [DOI] [PubMed] [Google Scholar]
- 151.Mcgregor A, Fox-Talbot K, Velidedeoglu E, Baldwin WMI, Wasowska BA. The absence of FcgRIII results in increased pro-inflammatory response in FcgRIII KO cardiac allograft recipients. Am J Transpl. 2009;9(s2):481. [Google Scholar]
- 152.Park-Min KH, Serbina NV, Yang W, Ma X, Krystal G, Neel BG, et al. FcgammaRIII-dependent inhibition of interferon-gamma responses mediates suppressive effects of intravenous immune globulin. Immunity. 2007;26:67–78. doi: 10.1016/j.immuni.2006.11.010. [DOI] [PubMed] [Google Scholar]
- 153.Clynes R. IVIG therapy: interfering with interferon-gamma. Immunity. 2007;26:4–6. doi: 10.1016/j.immuni.2007.01.006. [DOI] [PubMed] [Google Scholar]
- 154.Clynes R. Protective mechanisms of IVIG. Curr Opin Immunol. 2007;19:646–51. doi: 10.1016/j.coi.2007.09.004. [DOI] [PubMed] [Google Scholar]